![]()
NCC Certified EFM Dumps Questions Valid EFM Materials
Current EFM Exam Dumps [2026] Complete NCC Exam Smoothly
NEW QUESTION # 61
A woman is admitted to labor and delivery with vaginal bleeding. This tracing is obtained. This is most consistent with:
- A. Normal baseline
- B. Dysrhythmia
- C. An indeterminate pattern
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
The tracing shows:
* Baseline approx. 120 bpm
* Minimal variability (amplitude <5 bpm) across the entire strip
* No accelerations
* No decelerations
* Contractions present but not excessive
NCC defines:
* Category I requires moderate variability # not present.
* Category III requires absent variability with recurrent decels, bradycardia, or sinusoidal pattern # not present.
* Thus this falls into Category II: "indeterminate."
Minimal variability for this length of time cannot be considered a normal baseline, especially in the setting of vaginal bleeding, which raises concern for:
* Abruption
* Maternal anemia
* Hypovolemia
* Decreased uteroplacental perfusion
There is no evidence of dysrhythmia (no irregular R-R intervals, no chaotic spikes, no sawtooth pattern).
Therefore, the correct interpretation is A. An indeterminate pattern (Category II).
References:NCC C-EFM Candidate Guide; NICHD Definitions; AWHONN Principles & Practices; Menihan; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 62
This fetal heart rate tracing is from a woman in the second stage of labor. This tracing is best interpreted as: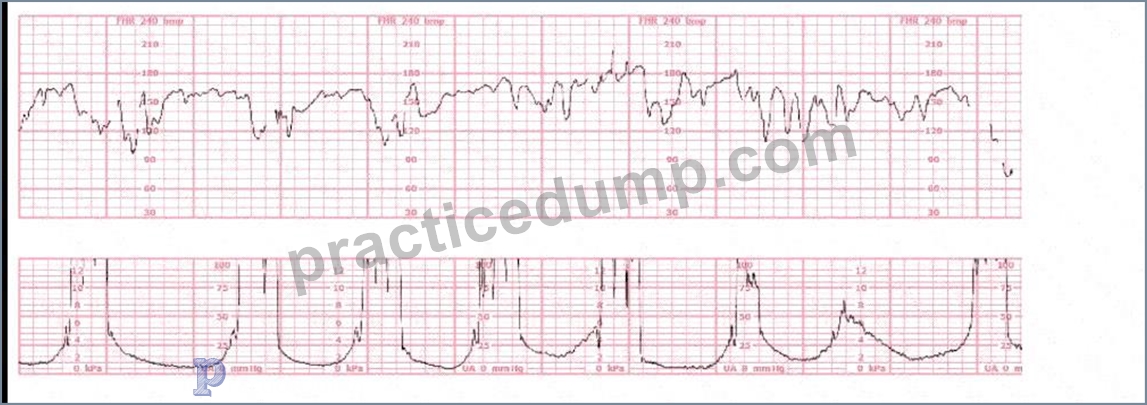
- A. Variable decelerations
- B. Wandering baseline
- C. Intermittent late decelerations
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
The tracing shows the classic features of variable decelerations:
* Abrupt onset (<30 seconds from baseline to nadir)
* Rapid drop followed by a rapid recovery
* Significant variability in shape, depth, and timing
* "Shouldering"-brief accelerations before or after the deceleration, typical of cord compression
* The decelerations vary in appearance and timing relative to contractions In second stage, this pattern is extremely common due to:
* Recurrent cord compression during descent
* Maternal pushing
* Reduced amniotic fluid with advancing labor
Why the other options are incorrect:
A). Intermittent late decelerations
* Late decelerations are uniform, smooth, begin after the contraction peak, and recover after the contraction ends.
* This tracing shows abrupt, variable-shaped, non-uniform decels # NOT late decels.
C). Wandering baseline
* A wandering baseline is a slowly fluctuating, low-amplitude, smooth, preterminal pattern.
* This tracing shows an identifiable baseline with variability and clear decelerations, not wandering baseline.
Thus, the tracing is most consistent with variable decelerations.
References:NCC C-EFM Candidate Guide; AWHONN FHMPP; NICHD FHR Definitions; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 63
Uterine contraction intensity is manually measured by degree of uterine:
- A. Muscle strength
- B. Pain
- C. Indentation
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Equipment Concepts:
When using external tocodynamometry, uterine contraction intensity cannot be measured in mmHg. It is assessed manually, using palpation. NCC and AWHONN teach:
* Contraction intensity is estimated by palpating the fundus during a contraction.
* The degree of firmness versus indentation determines intensity:
* Mild # uterus easily indented
* Moderate # firm, difficult to indent
* Strong # rigid, cannot be indented
Why the incorrect answers are wrong:
* B. Muscle strength - Not measurable by external or manual exam.
* C. Pain - Not a reliable indicator; pain perception varies widely and does not correlate with uterine intensity.
Thus, the correct manual measurement is done through uterine indentation, making A correct.
References:NCC C-EFM Candidate Guide; AWHONN Principles & Practices; Menihan EFM; Miller's Pocket Guide; Simpson & Creehan.
NEW QUESTION # 64
When a difference in interpretation occurs over a non-emergent electronic fetal heart rate tracing, the first step toward resolution is to:
- A. Follow the chain of command
- B. Document the incident in the medical record
- C. Have the involved clinicians review the tracing together
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
NCC's Professional Issues domain emphasizes communication, collaboration, and team-based interpretation of electronic fetal monitoring tracings.
For non-emergent differences in interpretation, the first step is:
* Discussion and joint review of the tracing by the involved clinicians.
Only if disagreement persists should the chain of command be used. Documentation occurs after consensus or escalation-not as the first step.
Thus, the appropriate first step is C. Have the involved clinicians review the tracing together.
References:NCC C-EFM Candidate Guide; AWHONN Standards for Professional Fetal Monitoring Practice; TeamSTEPPS principles.
NEW QUESTION # 65
The baseline fetal heart rate decreases with gestational age as a result of an increase in:
- A. Intrinsic ventricular rate
- B. Parasympathetic tone
- C. Catecholamine production
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
As gestation advances:
* Vagal (parasympathetic) control increases,
* Sympathetic dominance decreases,
* Resulting in a lower baseline heart rate.
NCC physiology teaching:
"Baseline FHR decreases with advancing gestational age due to maturation and increasing parasympathetic tone." Why the others are incorrect:
* Catecholamines increase heart rate, not decrease it.
* Intrinsic ventricular rate does not change significantly with gestational age.
Thus, the correct physiologic factor is increased parasympathetic tone.
References:NCC Physiology Domain; AWHONN; Menihan; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 66
(Full question statement)
Recurrent decelerations are defined as occurring with 50% or more of contractions in any window of how many minutes?
- A. 0
- B. 1
- C. 2
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract Without Links:
According to the NCC C-EFM Content Outline and AWHONN Fetal Heart Monitoring Principles, recurrent decelerations are specifically defined as decelerations that occur with #50% of uterine contractions in a
20-30-minute window, but standardized interpretation guidelines used by NCC and ACOG categorize recurrent patterns based on any 30-minute evaluation period.
AWHONN (FHM 6th Ed.) explains that fetal heart patterns must be evaluated over "a sufficiently long segment, typically 30 minutes, to determine whether the pattern is intermittent or recurrent." Menihan & Simpson further emphasize that recurrent decelerations imply a persistent physiologic stressor, requiring systematic evaluation and intrauterine resuscitation. NCC's Candidate Guide ties this rule directly into categorization within Category II and III tracings. Therefore, 30 minutes is the correct standard evaluation interval for determining recurrence.
NEW QUESTION # 67
The fetal heart rate baseline is
- A. normally between 110 and 170 beats per minute
- B. established between periodic and episodic changes
- C. documented in a 15 beats per minute range
Answer: B
Explanation:
Comprehensive and Detailed Explanation (From NCC C-EFM-Referenced Sources) The NCC C-EFM exam outline, along with AWHONN and Miller's Pocket Guide, define baseline fetal heart rate as the mean FHR rounded to increments of 5 bpm, measured over a 10-minute window, excluding:
* accelerations
* decelerations
* periods of marked variability
* any segments differing by >25 bpm
This aligns with ACOG, AWHONN, and Simpson's interpretation standards.
Option A is incorrect: the baseline is not documented as a 15-bpm range; it is documented as a single value (e.g., 140 bpm).
Option C is incorrect: the correct NCC/ACOG standardized normal baseline is 110-160 bpm, not 170.
Exact Extract Concepts Referenced:
- "Baseline is determined over a 10-minute period excluding periodic or episodic changes." (AWHONN FHR Principles)
- "Baseline is the mean FHR rounded to 5-bpm increments." (Miller's Pocket Guide)
- "Normal baseline is 110-160 bpm." (Simpson & Menihan; Creasy & Resnik)
NEW QUESTION # 68
When evaluating a baseline fetal heart rate change, the fetal heart rate is assessed for a minimum of:
- A. 15 minutes
- B. 10 minutes
- C. 30 minutes
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
NCC and NICHD define baseline FHR as the mean FHR rounded to increments of 5 bpm during a minimum of a 10-minute window, excluding:
* Accelerations
* Decelerations
* Marked variability
If a segment shorter than 10 minutes is used, it cannot be called a "baseline".
Thus the required minimum is 10 minutes.
References:NICHD Definitions; NCC C-EFM Candidate Guide; AWHONN; Miller's Pocket Guide.
NEW QUESTION # 69
When accelerations precede a variable deceleration pattern, this is caused by
- A. oligohydramnios
- B. hypoxic reflex response
- C. occlusion of the umbilical vein
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract (No URLs or Links) NCC-recommended physiologic texts (AWHONN, Menihan, Simpson, Creasy & Resnik) explain that variable decelerations are caused by umbilical cord compression. This process occurs in a three-step sequence, well known in fetal monitoring physiology:
* Umbilical vein occlusion occurs first # decreases fetal venous return # brief fetal acceleration (a compensatory sympathetic response).
* Umbilical artery occlusion follows # increases fetal systemic vascular resistance # variable deceleration as vagal stimulation lowers the fetal heart rate.
* Release of compression # post-deceleration acceleration may occur.
Thus, an acceleration immediately before a variable deceleration represents the initial compression of the umbilical vein, not a hypoxic response. This is a normal physiologic response to transient cord compression, often described in AWHONN and Menihan's physiologic explanation of "shoulders" around variable decelerations.
Oligohydramnios can contribute to cord compression but does not explain accelerations preceding the deceleration. A "hypoxic reflex" would not produce a pre-deceleration acceleration.
Therefore, the correct physiologic cause is:
Umbilical vein occlusion.
References (No URLs)
* NCC C-EFM Candidate Guide 2025 - Physiology
* AWHONN Fetal Heart Monitoring Principles
* Menihan: Electronic Fetal Monitoring
* Simpson & Creehan: Perinatal Nursing
* Creasy & Resnik: Maternal-Fetal Medicine
NEW QUESTION # 70
Fetal supraventricular tachycardia will often appear on the monitor as
- A. artifact
- B. the same rate as the maternal pulse
- C. half the actual rate
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources NCC-recommended fetal assessment texts emphasize that external Doppler ultrasound may undercount very rapid fetal arrhythmias such as fetal supraventricular tachycardia (SVT). Because Doppler detects mechanical motion rather than electrical activity, the device may record only every other cardiac contraction
, a phenomenon known as "half-counting."
Menihan's Electronic Fetal Monitoring explains that with SVT-often exceeding 200 to 260 bpm-the monitor "may display a fetal heart rate at approximately half the true atrial rate." AWHONN teaching materials affirm that rapid, regular tachyarrhythmias may appear deceptively slower on the external monitor due to Doppler under-sampling. Simpson & Creehan note that half-counting is a recognized technical limitation and may cause clinicians to miss true tachyarrhythmias if internal monitoring is not applied.
In contrast, artifact displays irregular, inconsistent, and non-physiologic deflections. Matching the maternal pulse suggests maternal heart rate misinterpretation, not SVT.
Miller's Pocket Guide also highlights that half-counting is "commonly seen in fetal SVT when using external Doppler due to failure to detect each rapid contraction." Therefore, fetal SVT most commonly appears as half the actual rate on an external fetal monitor.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesMenihan - Electronic Fetal MonitoringSimpson & Creehan - Perinatal NursingCreasy & Resnik - Maternal-Fetal MedicineMiller's Pocket Guide
NEW QUESTION # 71
During amnioinfusion, the infusion should be stopped periodically to assess changes in:
- A. Baseline uterine pressure
- B. Contraction pattern
- C. Patient pain level
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
During amnioinfusion, NCC emphasizes monitoring for uterine overdistention, which can lead to uterine hypertonus, uterine rupture, or placental separation. The primary way to evaluate overdistention is by measuring baseline uterine pressure via IUPC.
* Rising resting tone (>20-25 mmHg) indicates accumulating fluid and risk.
* Stopping the infusion intermittently allows recalibration and assessment of uterine baseline pressure.
* Contraction pattern (option B) is important but not the primary safety parameter.
* Pain (option C) is nonspecific and not a reliable indicator of uterine overdistention.
Thus, the infusion is stopped to assess baseline uterine pressure.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; Miller' s Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring.
NEW QUESTION # 72
This fetal heart rate pattern is classified as Category III based on: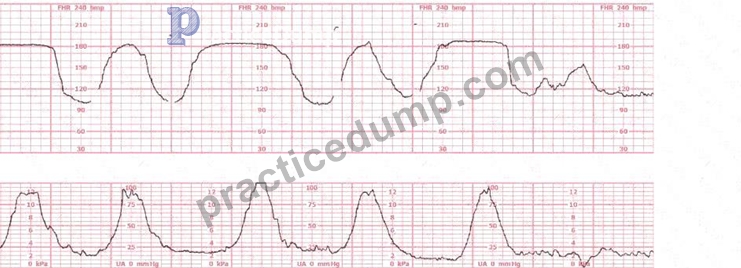
- A. Contraction pattern
- B. Type of deceleration
- C. Absent variability
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
This tracing shows recurrent late decelerations accompanied by absent variability.
Per NICHD/NCC, a tracing is Category III if ANY of the following are present:
* Absent variability AND recurrent late decelerations
* Absent variability AND recurrent variable decelerations
* Absent variability AND bradycardia
* Sinusoidal pattern
In this strip:
* Variability is absent
* Decelerations are recurrent and late
The determining feature for the classification is absent variability, which indicates significant risk for fetal acidemia.
The contraction pattern (option B) does not determine category.
The deceleration type alone (option C) does not determine Category III without absent variability.
Thus, the classification is Category III because of absent variability.
References:NCC C-EFM Candidate Guide; NICHD Three-Tier System; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring.
NEW QUESTION # 73
This tracing reflects: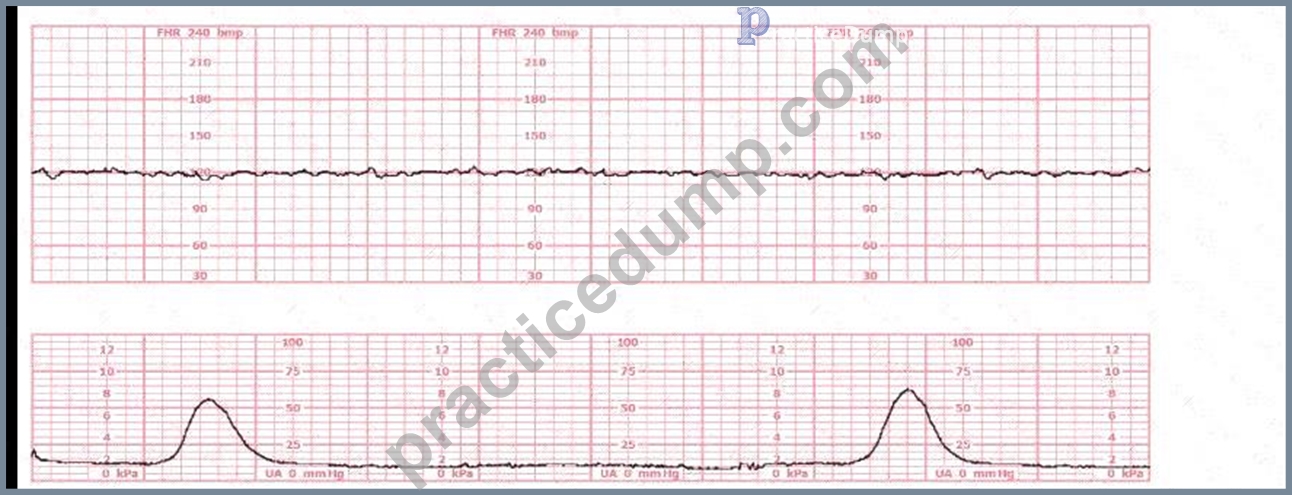
- A. Category I
- B. Category III
- C. Category II
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
In NCC C-EFM interpretation, classification of a fetal heart tracing is based on NICHD's three-tier system:
Category I, II, and III. Category III represents an abnormal tracing requiring immediate evaluation and prompt intervention.
Key findings in this tracing:
* Baseline:Baseline is approximately 140 bpm, within the normal range (110-160 bpm).Baseline alone does not determine category.
* Variability:The tracing shows absent variability:
* No beat-to-beat oscillations
* Flat, minimal fluctuationNICHD and NCC define absent variability as amplitude range undetectable.
* Accelerations:No accelerations are present.
* Decelerations:The strip does not show decelerations or bradycardia.However, absent variability alone with no accelerations for 20 minutes is highly concerning.
Category Classification per NICHD/NCC:
Category III criteria include ANY of the following:
* Absent variability with recurrent late decelerations
* Absent variability with recurrent variable decelerations
* Absent variability with bradycardia
* Sinusoidal pattern
Also recognized as Category III:
* Persistent absent variability lasting #20 minutes with no accelerations, which is strongly suggestive of fetal acidemia when sustained.
This tracing shows:
* Absent variability (flat line)
* No accelerations
* Persisting over an extended period
Under NCC and AWHONN guidance:
A persistently flat tracing must be classified as Category III unless proven otherwise (e.g., fetal sleep, maternal medications), and it requires immediate intrauterine resuscitation and evaluation for potential expedited delivery.
Why Category I is NOT correct:
Category I requires:
* Moderate variability
* No late or variable decelerationsThis tracing does not have moderate variability.
Why Category II is NOT correct:
Category II includes minimal variability, marked variability, intermittent variables/lates, absence of accelerations after stimulation.
This tracing is worse than Category II because variability is absent, not minimal.
Thus, the tracing fits Category III.
References:NCC C-EFM Candidate Guide (2025); NCC Content Outline; NICHD Three-Tier FHR Interpretation System; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 74
This fetal heart rate tracing is obtained upon the woman's admission to labor and delivery. This tracing is most reflective of: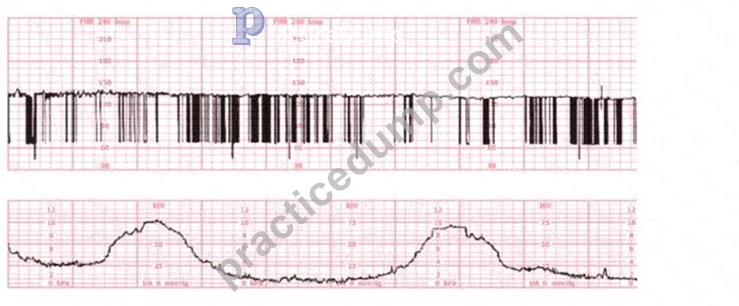
- A. Fetal dysrhythmia
- B. Atrial flutter
- C. Complete heart block
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
When evaluating an admission tracing, NCC emphasizes determining whether the pattern represents baseline variability abnormalities, signal artifact, or an underlying fetal cardiac rhythm disturbance. The strip shown contains clear features of a fetal dysrhythmia, which NCC and AWHONN describe as an irregular rhythm characterized by inconsistent R-R intervals or intermittent missed beats.
Key features in this tracing:
* Extremely irregular FHR signalThe pattern shows abrupt vertical spikes, inconsistent spacing, and intermittent loss of coherent waveform. NCC teaches that this appearance is typical of irregular ventricular conduction or premature atrial/ventricular contractions.
* Wide variability in beat spacingBeat intervals vary significantly, suggesting ectopic beats or conduction abnormalities rather than a stable rhythm such as heart block or atrial flutter.
* Sensor not malfunctioningThe lower uterine activity channel is smooth and consistent, meaning the upper channel's abrupt changes represent true FHR signal irregularity, not artifact.
Why the incorrect answers are ruled out:
A). Atrial flutter - NOT supported
* Atrial flutter produces a very fast, regular atrial rate (typically 300 bpm) with a repetitive saw-tooth pattern.
* It does not produce the highly irregular beat-to-beat pattern seen here.
* FHR in atrial flutter appears more organized, not chaotic.
B). Complete heart block - NOT supported
* Complete heart block (third-degree AV block) produces a very slow, regular ventricular rate, commonly 50-70 bpm, with a dissociation between atrial and ventricular rhythms.
* The tracing here does not show a slow, steady baseline.
* Instead, the rhythm is highly irregular with spikes and losses-not characteristic of AV block.
C). Fetal dysrhythmia - CORRECT
* NCC, AWHONN, Miller, and Menihan describe fetal dysrhythmias as:"Irregular, inconsistent FHR patterns due to premature atrial contractions (PACs), premature ventricular contractions (PVCs), or intermittent conduction disturbances."
* The hallmark is an irregular rhythm, often appearing as abrupt spikes or missing beats on the monitor.
* The tracing shown matches these characteristics precisely.
Therefore, the tracing is most consistent with fetal dysrhythmia, typically benign PACs/PVCs, and is the correct answer.
References:NCC C-EFM Candidate Guide (2025); NCC Content Outline; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 75
When documenting the occurrence of late decelerations in the medical record, what should be charted?
- A. Tracing category
- B. Components of the tracing
- C. Notation that the tracing was normal or abnormal
Answer: B
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
According to NCC, AWHONN, and evidence-based documentation standards, clinicians must document:
* Baseline
* Variability
* Accelerations
* Decelerations (type, depth, duration, timing)
* Uterine activity
This fulfills the NICHD 3-tier system and legal documentation expectations.
Why the incorrect answers are wrong:
* B. "Normal/abnormal" # vague, not an acceptable documentation standard.
* C. Category alone # insufficient; categories must be supported by the components.
References:NCC C-EFM Candidate Guide; AWHONN Documentation Standards; Menihan.
NEW QUESTION # 76
The ratio of oxyhemoglobin to the total amount of hemoglobin available is called oxygen
- A. saturation
- B. carrying capacity
- C. affinity
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources Oxygen saturation refers to the percentage of hemoglobin binding sites occupied by oxygen. NCC physiology resources, including Simpson & Creehan and Creasy & Resnik, define oxygen saturation as the
"ratio of oxyhemoglobin to total hemoglobin"-the same definition used in fetal oxygenation discussions.
Oxygen affinity refers to hemoglobin's tendency to bind oxygen (related to the oxyhemoglobin dissociation curve).
Oxygen carrying capacity refers to the total amount of oxygen hemoglobin can transport, independent of current saturation.
AWHONN and Menihan emphasize that fetal oxygenation assessment is dependent on understanding oxygen saturation, not affinity or carrying capacity, when discussing fetal hypoxemia and gas exchange.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesSimpson & Creehan - Perinatal NursingCreasy & Resnik - Maternal-Fetal MedicineMenihan - EFM ConceptsMiller's Pocket Guide
NEW QUESTION # 77
A woman has been 5 cm dilated for the past 3 hours. The tracing shown has developed over the last 30 minutes. The best initial course of action is to: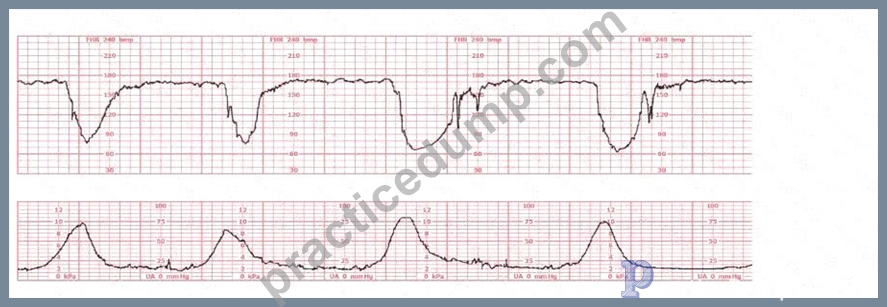
- A. Continue to monitor
- B. Proceed with cesarean section
- C. Perform intrauterine resuscitative measures
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
The fetal heart rate tracing demonstrates recurrent deep variable decelerations with a rapid drop in FHR, a V-shaped pattern, and slow return to baseline. These are classic signs of cord compression. According to NCC, AWHONN, Miller, Menihan, and Simpson, recurrent variable decelerations require immediate intrauterine resuscitative interventions before any decision regarding operative birth.
NCC-aligned intervention steps include:
* Maternal repositioning (first-line for cord compression)
* Reducing or stopping oxytocin if infusing
* IV fluid bolus
* Amnioinfusion (if appropriate and recurrent deep variables persist)
* Oxygen only if other measures fail (per NCC/AWHONN updated guidance)
The cervix has remained unchanged at 5 cm for 3 hours (a prolonged latent or early active labor pattern), but the fetal tracing shows Category II-recurrent variable decelerations. Category II dictates corrective action, not immediate delivery unless it progresses to Category III.
Cesarean birth (option C) is reserved for:
* Persistent Category III
* Failure of intrauterine resuscitation
* Proven fetal intoleranceNone of these conditions have been met yet.
Thus, the correct initial management is B. Perform intrauterine resuscitative measures.
References:NCC C-EFM Candidate Guide (2025); NCC Content Outline; NICHD FHR Definitions; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 78
Patient safety is enhanced when alarms:
- A. Occur infrequently
- B. Are determined by the unit leaders
- C. Can be called by anyone
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NCC and AWHONN emphasize unit-wide shared responsibility for:
* Recognizing abnormal maternal or fetal findings
* Calling for help
* Triggering emergency responses (e.g., unit huddle, rapid response, safety pathways) Safety culture requires:
* Any staff member (RN, tech, provider) to initiate an alarm or escalate concern
* No hierarchy delay
* Rapid action when fetal compromise is suspected
Why the other answers are wrong:
* A. Determined by unit leaders # incorrect; safety is team-wide, not hierarchical.
* C. Occur infrequently # false; alarms must occur whenever needed, not limited.
Correct answer: B. Can be called by anyone.
References:NCC Professional Issues Domain; AWHONN Standards for Professional Practice; Perinatal Safety Bundles; Simpson & Creehan.
NEW QUESTION # 79
A fetal heart rate pattern characteristic of fetal neurological injury and impending intrapartum fetal demise is:
- A. Wandering baseline
- B. Recurrent late decelerations
- C. Marked variability
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
A wandering baseline is:
* A slow, fluctuating baseline
* Low amplitude
* No variability
* No accelerations
* Indicative of severe fetal neurologic injury and terminal fetal status NCC and AWHONN describe wandering baseline as a preterminal pattern.
Why the other answers are wrong:
* A. Marked variability # often transient and not associated with demise.
* B. Recurrent lates # concerning but not a neurological-injury pattern unless variability absent.
Correct answer: C. Wandering baseline.
References:NCC Pattern Recognition; AWHONN FHMPP; Menihan; Simpson & Creehan.
NEW QUESTION # 80
Nonstress testing is used more frequently for antepartum testing than contraction stress testing because contraction stress testing has a:
- A. Low predictability of fetal well-being within 7 days of a negative test
- B. Higher frequency of equivocal test results
- C. Limited reporting option for the compromised fetus
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
NCC and AWHONN explain that Contraction Stress Testing (CST):
* Has a higher rate of equivocal ("equivocal-suspicious" or "equivocal-hyperstimulation") results
* Frequently must be repeated or replaced with other tests
* Requires inducing contractions, which carries risk (hyperstimulation, preterm labor, uterine rupture in scarred uterus) NST is used more commonly because it is:
* Noninvasive
* Easier to perform
* Has fewer contraindications
* Has a lower rate of equivocal results
Why the others are incorrect:
* B - CST does detect fetal compromise reliably and is NOT limited in its reporting structure.
* C - A negative CST actually has very high negative predictive value for 7 days, making this answer incorrect.
Thus the correct choice is A. Higher frequency of equivocal results.
References:NCC C-EFM Candidate Guide; AWHONN; Menihan; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 81
A woman (G1P0) arrives in triage with a pain score of 4/10 at 39-weeks gestation. The fetal heart rate tracing shown is obtained. The best intervention is to:
- A. Adjust tocotransducer and continue to monitor
- B. Admit for induction
- C. Discharge to home
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
This tracing demonstrates a normal, reassuring fetal heart pattern that is technically categorized as Category I, indicating normal fetal acid-base status. Before any decision regarding discharge or induction, NCC emphasizes correct assessment of the tracing quality, fetal status, and uterine activity.
Key Tracing Characteristics
* Baseline:Approximately 135-145 bpm, well within the normal range of 110-160 bpm.
* Variability:The strip shows moderate variability (6-25 bpm), the strongest indicator of adequate fetal oxygenation per NCC, AWHONN, and NICHD.
* Accelerations:Several accelerations are present-another reassuring feature of normal fetal well-being.
* Decelerations:No variable, late, or prolonged decelerations are present.
* Uterine Activity:The lower channel shows poor recording quality and inconsistent signal- suggesting the toco is not capturing contractions well, not that the patient is contracting excessively or not at all.
Correct interpretation per NCC:
NCC emphasizes distinguishing between physiologic assessment and technical artifact.
The fetal tracing is completely reassuring.
The only abnormality is the poor uterine activity signal, a common triage occurrence due to:
* Toco placement
* Maternal body habitus
* Positioning
* Low contraction intensity in early labor
Thus, the correct next step is to optimize equipment (reposition the toco, adjust belt, palpate contractions) and continue to monitor.
Why the other options are incorrect:
B). Admit for induction - NOT indicated
* There is no evidence of fetal compromise.
* No indication for induction is present (pain score 4/10, reassuring FHR, term pregnancy).
* NCC emphasizes avoiding unnecessary interventions.
C). Discharge to home - NOT yet appropriate
* You cannot safely discharge a patient with a poorly monitored contraction pattern.
* Adequate assessment requires confirming uterine activity-after fixing the toco.
Therefore, the appropriate action is:
A). Adjust tocotransducer and continue to monitor.
References:NCC C-EFM Candidate Guide (2025); NCC Content Outline; AWHONN Fetal Heart Monitoring Principles & Practices; NICHD Definitions; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 82
In documenting auscultation of the fetal heart rate, it is important to record findings in relationship to:
- A. Uterine activity
- B. Fetal position
- C. Stage of labor
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NCC and AWHONN auscultation standards emphasize the need to document FHR findings relative to uterine contractions, including:
* The FHR between contractions (baseline)
* FHR during contractions
* Presence/absence of decelerations
* Recovery after a contraction
Uterine activity determines whether findings are:
* Baseline
* Accelerations
* Early/late/variable decelerations
Why the other options are incorrect:
* A. Fetal position - relevant for Doppler placement, not auscultation documentation.
* B. Stage of labor - affects monitoring frequency but does not change how findings are documented.
Correct answer: C. Uterine activity.
References:NCC C-EFM Candidate Guide; AWHONN Standards for FHR Auscultation; Simpson & Creehan.
NEW QUESTION # 83
......
EFM Premium PDF & Test Engine Files with 127 Questions & Answers: https://certkingdom.practicedump.com/EFM-practice-dumps.html